How did tobacco and smoking become a global health policy issue? This article – the third in our series (1, 2) on non-communicable diseases (NCDs) – examines the critical juncture at which new information, new information technology and an emergent transnational activism combined to produce a new agenda for reducing the impact of NCDs.

Health hazards of smoking in 1824: the flaming moustache
(Detail from “Corinthian Steamers”. Source: Wikimedia Commons)
Once upon the time, the multi-billion dollar tobacco industry appeared legally impregnable, and held enough sway to turn United Nations (UN) organisations against the World Health Organisation (WHO) to neutralise global tobacco control efforts.
A 1999 World Bank report estimated that four million people died annually from tobacco-related illnesses and predicted the number to rise to ten million by 2030, with 70% of these deaths occurring in “developing” countries. According to Taylor and Bettcher, 800 million of the 1.25 billion smokers worldwide lived in developing countries in 2000.
However, within the emerging global health community, a transnational anti-tobacco movement was gaining momentum by the late 1990s. One major shift in approach by the WHO was the development of a new anti-smoking initiative within its new commitment to non-communicable diseases (NCDs). NCDs increasingly became a legitimate area of WHO involvement, which was concerned about tobacco as the second leading NCD risk factor, causing 9% of mortality worldwide.
In this context, a 1998 trial between the US state of Minnesota and the tobacco giant Philip Morris became a watershed for the movement by making available classified documents which catalysed a transnational push for new regulation; in particular, the WHO’s campaign against tobacco-related illnesses. According to medical researchers:
The use of these documents in furthering public health goals based in science, policy, and litigation—the 3 fronts on which the tobacco industry had successfully escaped accountability for decades—has been nothing short of astounding. (Hurt et. al. 2009)
The emergence of the global anti-tobacco movement, which capitalized on this new informational resource, catalyzed the broader formation of the transnational campaign against NCDs. Below, we trace the progression of anti-tobacco campaigns from the early 1990s to the adoption of the WHO Framework Convention on Tobacco Control (FCTC) in 2003. The FCTC is the world’s first public health treaty, the only time in history that the WHO used its litigation powers, and one of the first multilateral and binding agreements related to an NCD.
Growth first, health later
For much of the second half of the twentieth century, the tobacco industry still enjoyed support from major financial organisations such as the World Bank and the International Monetary Fund within their broader development agenda. Even in 1986, to the backdrop of traditional-sounding music, a promotional video by the British American Tobacco Company (BATCo) could claim:
For the growers in Asia, Africa and Latin America, tobacco is the key to a better life. BATCo companies provide farmers with a guaranteed market for their crop at competitive prices and all the backup they need to improve their agricultural skills.

BATCo promotional video, 1986 (click to play externally)
Yet from the 1970s on in the wealthier parts of the world, public recognition of the health hazards of smoking rose, accompanied by higher taxes on tobacco products. Consequently, cigarettes consumption declined in most wealthy countries.
In sharp contrast to richer countries, however, from 1970 to 2000 tobacco consumption in developing countries increased rapidly. Unhindered by anti-smoking movements, consumption increased annually on average by 5%; by 2000, aggregate consumption had risen by 70%. According to the United Nations Food and Agricultural Organisation (FAO), this increase, which occurred everywhere in the developing world, was particularly buoyed by the formidable populations of China and India. Philip Morris’ 1997 Annual Report saw investment opportunities ‘larger than ever.’
But at the same time academia and advocates within non-government organisations (NGOs) were beginning to draw attention to a link between health improvements and positive economic effects, and calling for efficient national regulatory environments and harmonization of national policies between countries. In 1996 Chen et. al. noted health movements worldwide were verging on a “global health village.”
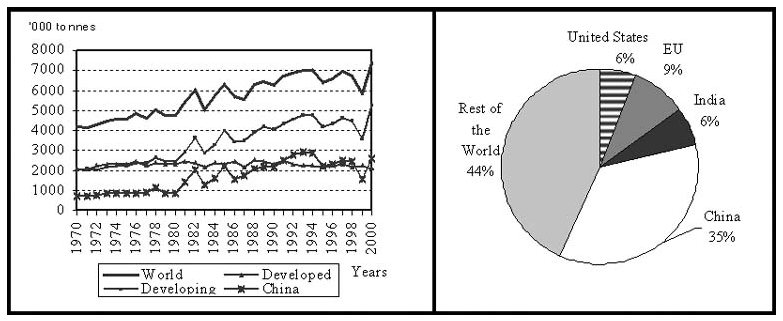
World tobacco consumption trends: developing countries rise after 1980, activism kicks in in the 1990s.
The 1999 World Economic Forum in Davos on “Responsible Globality” saw Gro Harlem Brundtland, Director-General of the WHO, arguing that tobacco was a major threat to public health globally. By October 2000 The Economist was reporting: ‘The tobacco war goes global’.
Seventy million confidential pages
This “global war” on tobacco was catalyzed by the outcome of a 1998 trial between Minnesota against Philip Morris. The state of Minnesota sued the major tobacco companies among other wrongdoings for conspiracy, fraud, and deliberately targeting youth. According to a May 1998 article from the Los Angeles Times, the terms of settling the lawsuit included US $ 6.6 billion in damages, halting payments to movie, television and video producers for featuring tobacco products, and dismantling the Council for Tobacco Research, which was alleged to have played a central role in spreading disinformation about health effects from smoking.
Yet another, and perhaps more lasting, legacy of the trial was the release of approximately seventy million confidential pages of documents, thousands of audiovisual files and hundreds of other electronic media. As Hurt et. al. explain: ‘No other comparable dynamic, voluminous, and contemporaneous document archive exists.’
The documents showed how the tobacco industry had undertaken extensive public relations campaigns to spread doubts about the connection between smoking and poor health, ‘but without actually denying it.’ Moreover, whilst the industry had previously argued that governments were controlling consumer choice, the documents revealed a concerted effort by the tobacco industry to market the virtues of freedom and individual choice along with their products.
Such revelations led WHO Director General Brundtland to launch an inquiry into the nature and extent to which the tobacco industry had sought to obstruct the WHO and other UN organisations’ efforts for tobacco control. It emerged that in 1993, INFOTAB, a think tank supported by the tobacco industry, had scrutinised the WHO’s programme budget and hired academics to spread doubt about the WHO’s priorities.
For example, Paul Dietrich, an American lawyer, and Robert Tollison, then director at the Centre for Study of Public Choice, were paid by BATCo to attack the WHO. They argued that WHO ‘spending should be concentrated on fighting diseases in third world nations, leaving rich, first world nations to finance their own programs.’ The tobacco industry had actively engaged in efforts to keep NCDs off transnational public health agendas. As Yach and Bettcher explain, WHO funds would thus continue to fight malaria and cholera, ‘but not go for the campaigns for seat belts or against cigarettes and alcohol.’
Such revelations from the 1998 trial were damaging for the industry’s public reputation, and they stimulated global action against what was now being referred to as the ‘tobacco epidemic’.
Control of the agenda shifts from industry to activists and WHO
The 1998 trial also revealed a tobacco industry worried about the opportunities for activism in a globalizing world connected by new information technology. When the Union for International Cancer Control (UICC) was setting up GlobaLink in 1992, a major non-profit alliance connecting NGOs in the fight against cancer worldwide, an American spokesman for the Tobacco Institute (a now dissolved US industry trade group) warned the Institute’s South African affiliate:
Through a worldwide computer network established by the Washington DC based Advocacy Institute anti-tobacco activists now are able to transmit media advisories, reactions and proposed sound bites on virtually any smoking related issue to colleagues in other countries, and to the press. I have told our members that I believe that this expanding, sophisticated infrastructure is probably one of the greatest challenges our industry has confronted.
Such letters and correspondence between parent tobacco companies and foreign subsidiaries provided valuable insights into the efforts of transnational tobacco companies to curb activism, and upon release were used by tobacco control activists and movements. Governments such as Brazil, Austria, Nigeria and the UK used the documents in developing new tobacco-related policies. Moreover by 2000, lawsuits against the tobacco industry had been filed by Australia, Bangladesh, Brazil, Canada, China, Finland, France, Germany, India, Ireland, Israel, Japan, the Marshall Islands, Norway, Oman, Pakistan, Peru, Poland, South Korea, Spain, Sri Lanka, Switzerland, Uganda, and the United Kingdom
The Minnesota vs. Philip Morris trial helped shape a consensus among policy makers, governments and researchers about the tobacco industry as the ‘underlying cause’ of a significant increase in tobacco-related ailments. It thereby carved out one of the key channels through which preventive efforts against NCDs would proceed.
A major public health achievement: the Framework Convention
As explained by Douglas Blanke, former Assistant Attorney General of the US State of Minnesota: ‘The disclosures unleashed by the Minnesota documents lit a fire of indignation that helped drive […] the WHO’s Framework Convention on Tobacco Control.’ In May 1999 – exactly one year after the trial – the World Health Assembly unanimously adopted resolution WHA52.18, which initiated the FCTC: a significant move, as for most of the 1990s observers had criticised that ‘there is nothing bold…in [the] WHO’s approach to the tobacco industry.’
The FCTC was the first time the WHO employed its constitutional mandate to facilitate an international convention on global health and tobacco control. Officially established in 2003, the mandate of the FCTC ‘requires parties to adopt a comprehensive range of measures designed to reduce the devastating health and economic impacts of tobacco.’
According to Mallet, the FCTC was ‘one of the most rapidly and widely embraced treaties in the UN history.’ Former Surgeon General of the United States C. Everett Koop evaluated the treaty as one of the greatest public health achievements of the twentieth century. To date, the FCTC has been signed by 168 countries and is legally binding in 177 countries that ratified the treaty. The United States (under President George W. Bush) signed but did not ratify the Convention.
(eloise)



1 comment
Comments feed for this article
July 23, 2013 at 12:01
Peter
Great stuff Elle. As an avid non-smoker, I will pass this on