You are currently browsing the category archive for the ‘Global Health Governance’ category.
As we have all experienced recently, to prevent pandemic outbreaks or mitigate an evolving pandemic crisis, it is of utmost importance to guarantee timely and global access to safe and effective vaccines. Through their pre-print, Milena Leybold (University of Innsbruck) and Konstantin Hondros (University of Duisburg-Essen) make a step towards opening a debate on “Increasing Vaccine Access in a Shorter Time. Alternative Regulatory Frameworks in Response to Pandemics.”
Konstantin Hondros & Milena Leybold

Just over a year ago, Milena Leybold and Leonhard Dobusch asked, Why is there no open-source vaccine against Covid-19? and discussed arguments why open-source vaccines are difficult to achieve. In March 2022, The Financial Times published an article by Donato Paolo Mancini, Jamie Smyth, and Joseph Cotterill asking Will ‘open-source’ vaccines narrow the inequality gap exposed by Covid? (behind a subscription barrier) and indicating that the landscape of open-source vaccines may have changed substantially.This blog post is thought of as a reply and extension to this very informative report that introduces mainly two organizations producing or aiming to produce open-source vaccines: Afrigen Biologics and Vaccines (Afrigen) and the Texas Children’s Hospital Center for Vaccine Development (CVD with their vaccine Corbevax). For sure, Afrigen and CVD approach vaccine development, production, and distribution much more openly than most of the vaccines dominating the market. Still, it is unclear to what extent they should be considered as “open-source.” To clarify this topic, we scrutinize what an open-source vaccine ideally could be, to what degree Afrigen or CVD fit the ideals of open-source, and what other attempts for open-source vaccine alternatives are currently under development.
Read the rest of this entry »This post is provided by Suela Simoni, Student Assistant at Innsbruck University
While the concept of “open source” emerged as a radically open and transparent way of developing software, it is increasingly applied in other contexts as well. In pharmaceutical open source projects, for example, anyone can contribute at any time to the project, methods and data are in the public domain, and data is released as soon as it is acquired. However, compared to the software industry, open source approaches struggle to take ground in the pharma industry. As of December 2021 there has not been a single molecule worldwide, which has been discovered, developed, and brought to market completely open source. There are a few examples of patent-free molecules that have been going through clinical trials: one is the Praziquantel and the second one is the Fexinidazole. Since only a part of the process has been done openly in these cases, they cannot be considered to be completely ‘open source’. Using the example of the initiative “Open Source Malaria” and outlining the challenges they face, I will discuss why developing drugs and vaccines based on open source principles represents a difficult endeavor.
Read the rest of this entry »Building upon a case study of the Medicines Patent Pool, this blogpost aims to set the Medicines Patent Pool/Merck License for Molnupiravir in a processual context.
About the License Agreement
Recently, on October 27, 2021, the Merck & Co., Inc. Kenilworth NJ USA (MSD) and the Medicines Patent Pool (MPP) jointly announced the signing of a license agreement for Molnupiravir. Molnupiravir is an “an investigational oral antiviral medicine“ against Covid-19 that has shown promising results in Phase 3 clinical trials. The drug is currently under review by the European Medicines Agency (EMA). The voluntary license and technology transfer agreement for Molunpiravir allows generic manufacturers from anywhere in the world to produce the drug and supply it to 105 low-and middle income countries (the “territory”). Manufacturers can license royalty free for the time of the pandemic.
While the medical non-governmental organization Médecins Sans Frontières (MSF) criticizes the agreement for excluding “half of the world’s population and important upper-middle-income countries (UMICs) with robust manufacturing capacity, such as Brazil and China”, other medicine policy experts such as James Love or Peter Maybarduk celebrate the agreement as an “impressive achievement” or a “starting point and an example” to increasing access to Covid-19 therapies in LMICs. James Love commented that the “licensed area is large enough (more than half the world’s population) to induce efficient generic entry and economies of scale”.
To understand the impacts of this license agreement, we take a closer look on the patent pool mechanism that is leveraged here.
Read the rest of this entry »This post is provided by Jasmin Schmitz, Research Assistant at the Käte Hamburger Kolleg / Centre for Global Cooperation Research
When the then novel Covid-19-virus broke out in December 2019, it soon spread globally posing a challenge to health governance all across the globe. Internal containment measures were put in place to domestically stop the virus through lockdown or social distancing; internationally borders were closed, and travel restrictions were put in place to stop the ongoing spread at the borders. When first news broke that vaccine-trials were showing promising results, this seemed like the salvation from ever increasing new infections. Already during the first wave of Covid outbreaks trends of nation-focused policies could be observed. While there are certainly cases of cross-border cooperation, they tend to remain the exception. The WHO tried to install a global distribution mechanism through COVAX yet the initiative did not succeed in gaining global influence; Vaccine nationalism became is predominant mode of governance. The access to the shot has become highly dependent on where one lives. The inequality in access to vaccines has sparked discussion surrounding intellectual property as well as the involvement of public financing in the developmental stage of the pharmaceutical. So, more than half a year since the roll-out of the immunization campaign started, it is time to take a look at the distribution of vaccines globally and why they should not be viewed as the sole solution to the pandemic.
Read the rest of this entry »The Covid-19 pandemic is, without doubt, one of the biggest societal challenges of our times. Since its outbreak in December 2019, more than 3 million people died due to or with a Covid-19 infection. The pandemic hits the world with disastrous side effects such as economies suffering from recurrent or constant lockdowns, children who can’t go to school, or rising case numbers of mentally ill people. The most promising solution to stop the pandemic: vaccination.
In December 2020, the first person got vaccinated with the officially authorized Pfizer/BioNTech mRNA vaccine “COMIRNATY” in UK and Russia started mass vaccination with the vaccine “Sputnik V”. Shortly after, other big pharmaceutical companies such as Moderna, Astrazeneca, Sinovac, or Johnson & Johnson managed to get marketing authorizations for their vaccines. However, the vaccination campaigns proceed slower than expected: the demand for vaccines exceeds the production capacities of the pharma companies. Further, vaccines are not globally distributed at comparable rates. Unequal access to vaccines is not just a matter of injustice but imbalances also increase the risk of mutations developing in non-vaccinated countries.

Source: https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html
In January 2021, WHO Director-General Tedros Adhanom Ghebreyesus described the imbalance of vaccine distribution as “a catastrophic moral failure” and asked countries of the Global North to lift intellectual property protections so that countries around the world could produce vaccines. Similarly, the People’s Vaccine Alliance proposes offering the Covid-19 vaccine as a common good:
Our best chance of all staying safe is to ensure a COVID-19 vaccine is available for all as a global common good. This will only be possible with a transformation in how vaccines are produced and distributed — pharmaceutical corporations must allow the COVID-19 vaccines to be produced as widely as possible by sharing their knowledge free from patents.
https://peoplesvaccine.org
Instead they are protecting their monopolies and putting up barriers to restrict production and drive up prices, leaving us all in danger. No one company can produce enough for the whole world. So long as vaccine solutions are kept under lock and key, there won’t be enough to go around. We need a People’s Vaccine, not a profit vaccine.
This raises the question of this blog post: wouldn’t it be possible to organize the development of an open source vaccine that could be produced and distributed all over the world? Fortunately, media articles and governmental statements provide us with a rich bunch of arguments, why this is not an option. Let’s have a look at those.
Read the rest of this entry »How did tobacco and smoking become a global health policy issue? This article – the third in our series (1, 2) on non-communicable diseases (NCDs) – examines the critical juncture at which new information, new information technology and an emergent transnational activism combined to produce a new agenda for reducing the impact of NCDs.

Health hazards of smoking in 1824: the flaming moustache
(Detail from “Corinthian Steamers”. Source: Wikimedia Commons)
Once upon the time, the multi-billion dollar tobacco industry appeared legally impregnable, and held enough sway to turn United Nations (UN) organisations against the World Health Organisation (WHO) to neutralise global tobacco control efforts.
A 1999 World Bank report estimated that four million people died annually from tobacco-related illnesses and predicted the number to rise to ten million by 2030, with 70% of these deaths occurring in “developing” countries. According to Taylor and Bettcher, 800 million of the 1.25 billion smokers worldwide lived in developing countries in 2000.
However, within the emerging global health community, a transnational anti-tobacco movement was gaining momentum by the late 1990s. One major shift in approach by the WHO was the development of a new anti-smoking initiative within its new commitment to non-communicable diseases (NCDs). NCDs increasingly became a legitimate area of WHO involvement, which was concerned about tobacco as the second leading NCD risk factor, causing 9% of mortality worldwide.
Thirteen years ago the largest-ever gathering of world leaders took place on 8 September 2000 at the United Nations (UN) General Assembly in New York, where the UN Millennium Declaration was made. The Declaration was the most supported, ambitious and specific list of global development goals agreed upon to date, and established a list of commitments to reduce extreme poverty by 2015 which became known as the Millennium Development Goals (MDGs).

The Millennium Development Goals set in 2000
Source: United Nations
The MDGs were significant for global development cooperation due to their ability to stimulate global support, specifically financial resources. Many aid agencies and donors used them to direct their funding projects, and several governments also largely founded their health strategies upon them to receive external funding, which could comprise over 50 per cent of the state’s health budget. The MDGs thereby created a specific global development agenda, which some critics however now argue was not entirely in tune with the real needs of development of low- and middle-income countries. For example, proponents of a greater focus on non-communicable diseases (NCD) criticise that despite NCDs are now the leading cause of death worldwide, they did not receive a single mention in the 2000 MDGs.
Historically, infectious diseases such as HIV/AIDS, Tuberculosis and Malaria have been at the center of global health initiatives, as they easily spread across national borders and threatened the lives of millions of people in low- and middle-income countries with under-developed health care systems. Yet as the world celebrates its progress on the reduction of infectious diseases, the globalisation of unhealthy lifestyles, rapid and unplanned urbanisation, and liberal market forces have propelled a possibly greater threat to the health and development of the Global South, organisations like the World Health Organisation (WHO) fear. This threat is often referred to as “the invisible epidemic” of non-communicable diseases (NCDs), yet strategies on how to overcome them still remain unclear.
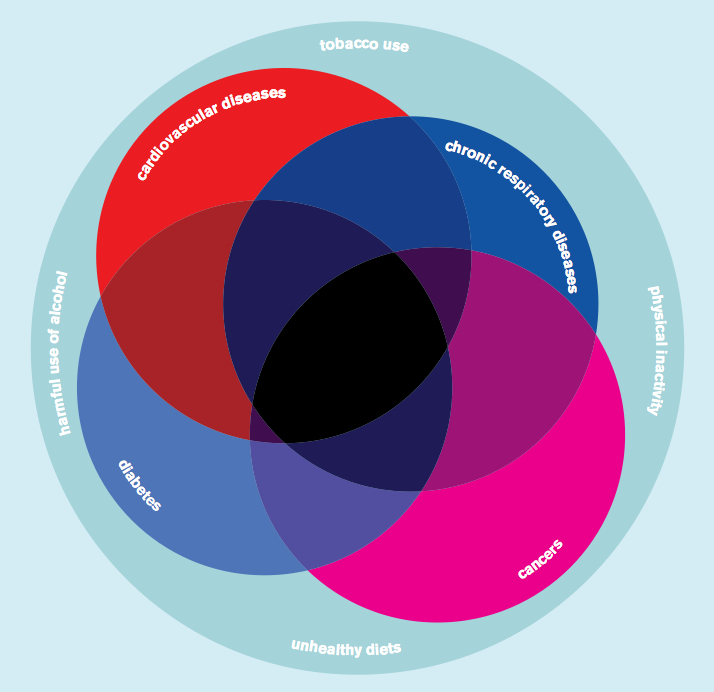
Causes and effects of non-communicable diseases
Source: World Health Organization
This blog entry is the first in a series of contributions exploring the rise of NCDs as a major health and development issue in low- and middle-income countries. The aim is to present and discuss evidence of the leading actors who are increasingly seeing NCDs not only as a challenge for developing countries, but also as an issue of transnational health governance that cannot be resolved at the national level alone. Read the rest of this entry »


